Back to B6 home
B6 F) Genetic Conditions
B6 F) Genetic Conditions
The content in this section builds on the content that was discussed in the previous section. Therefore, make sure that you have covered the content in the previous section before covering the content in this section (click here to be taken to the previous section).
We are going to look at 2 different genetically inherited disorders in this section; cystic fibrosis and polydactyly. Cystic fibrosis is caused by a recessive allele and polydactyly is caused by a dominant allele.
We are going to look at 2 different genetically inherited disorders in this section; cystic fibrosis and polydactyly. Cystic fibrosis is caused by a recessive allele and polydactyly is caused by a dominant allele.
Cystic Fibrosis
Cystic fibrosis is a genetic disorder that causes mucus to build up in the lungs and digestive system (we will be looking at cystic fibrosis in a little bit more detail in the mutation section). Cystic fibrosis is caused by a recessive allele and the notation for this recessive allele is usually f. This means that an individual will only have cystic fibrosis if they are homozygous recessive (ff).
Individuals who have the dominant allele (F) will not have cystic fibrosis. If an individual has the dominant allele and the recessive allele, they will not have cystic fibrosis and are known as being a carrier; the genotype of a carrier is Ff, which is heterozygous. If two carriers have a baby, there is a 1 in 4 chance that their offspring will have cystic fibrosis despite both parents not having cystic fibrosis.
We are now going to draw the Punnett square for two carriers having a child. As the parents are carriers, they will both have the genotype Ff, which means that they will both produce gametes that are F and f. The completed Punnett square is shown below.
Cystic fibrosis is a genetic disorder that causes mucus to build up in the lungs and digestive system (we will be looking at cystic fibrosis in a little bit more detail in the mutation section). Cystic fibrosis is caused by a recessive allele and the notation for this recessive allele is usually f. This means that an individual will only have cystic fibrosis if they are homozygous recessive (ff).
Individuals who have the dominant allele (F) will not have cystic fibrosis. If an individual has the dominant allele and the recessive allele, they will not have cystic fibrosis and are known as being a carrier; the genotype of a carrier is Ff, which is heterozygous. If two carriers have a baby, there is a 1 in 4 chance that their offspring will have cystic fibrosis despite both parents not having cystic fibrosis.
We are now going to draw the Punnett square for two carriers having a child. As the parents are carriers, they will both have the genotype Ff, which means that they will both produce gametes that are F and f. The completed Punnett square is shown below.
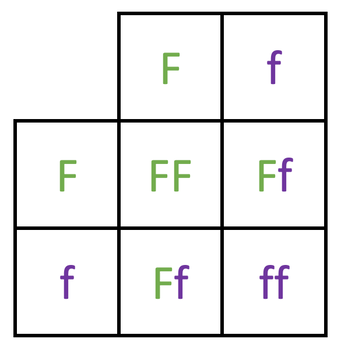
From looking at the outcomes of the Punnett square, we can see that there is 1 homozygous dominant (FF), 2 heterozygous (Ff) and 1 homozygous recessive (ff). Cystic fibrosis is caused by a recessive allele, which means that an individual will only have cystic fibrosis if their genotype is homozygous recessive (ff). Therefore, only 1 out of the 4 offspring has cystic fibrosis. Also, 2 of the offspring will be carriers; the heterozygous (Ff) will be carriers.
Polydactyly
Polydactyly is a genetic disorder where a baby is born with extra digits (extra fingers or toes). It is caused by a dominant allele which we generally denote as D. Therefore, an individual will have polydactyly if they are homozygous dominant (DD) or heterozygous (Dd). The only way that an individual will not have polydactyly is if their genotype is homozygous recessive (dd).
We are now going to have a question.
Question
A heterozygous individual and an individual who does not have polydactyly have a child. What is the percentage chance of the offspring having polydactyly?
The question tells us that one of the parents is heterozygous and the other parent does not have polydactyly. The genotype for the heterozygous parent will be Dd. The other parent does not have polydactyly and the only way that an individual cannot have polydactyly is if they are homozygous recessive; their genotype must be dd.
We now have the genotype of both parents; Dd and dd. The Punnett square is drawn below.
Polydactyly is a genetic disorder where a baby is born with extra digits (extra fingers or toes). It is caused by a dominant allele which we generally denote as D. Therefore, an individual will have polydactyly if they are homozygous dominant (DD) or heterozygous (Dd). The only way that an individual will not have polydactyly is if their genotype is homozygous recessive (dd).
We are now going to have a question.
Question
A heterozygous individual and an individual who does not have polydactyly have a child. What is the percentage chance of the offspring having polydactyly?
The question tells us that one of the parents is heterozygous and the other parent does not have polydactyly. The genotype for the heterozygous parent will be Dd. The other parent does not have polydactyly and the only way that an individual cannot have polydactyly is if they are homozygous recessive; their genotype must be dd.
We now have the genotype of both parents; Dd and dd. The Punnett square is drawn below.
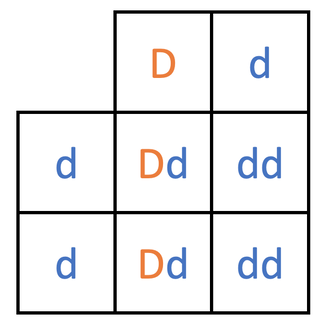
From the Punnett square, we can see that 2 of the offspring are heterozygous (Dd) and 2 of the offspring are homozygous recessive (dd). Polydactyly is caused by a dominant allele, which means that the 2 heterozygous offspring will have polydactyly. The 2 offspring that are homozygous recessive will not have polydactyly. Therefore, 2 out of the 4 offspring have polydactyly, which means that the percentage chance that the offspring will have polydactyly is 50%.
Screening Embryos
We can screen embryos to detect whether the embryos have any genetic disorders such as cystic fibrosis. The screening of embryos involves taking a few cells from the embryo and analysing the genetic information to see if there are any genes for genetic disorders present. We can screen embryos from IVF (fertilisation in a lab) and from embryos in a womb.
If the embryos do have any genetic disorders, the embryos from IVF will probably be destroyed and the embryos inside a womb may be terminated (the pregnancy will end and a child won’t be born). It is because of these reasons that the screening of embryos is extremely controversial, especially amongst religious individuals who believe that life starts when a sperm and an egg fuse together to form an embryo; these individuals probably class the implications of embryo screening (destroying the embryo during IVF and terminating a pregnancy) as murder. Also, the screening of embryos implies that some genetic disorders are undesirable, which creates conflict and prejudice. Furthermore, individuals may want to screen the embryos for more than just genetic disorders; for example, screening the embryos for hair colour, eye colour etc… However, at the moment there are laws that prevent this from happening; currently, parents cannot even know the sex of the offspring (unless the sex influences the health of the offspring). A final negative is that screening embryos is quite an expensive process.
The positives of embryo screening are that genetic disorders reduce the quality of life for many individuals. Therefore, embryo screening can prevent babies being born with genetic disorders, which can reduce suffering. Furthermore, the treating of these genetic disorders is very expensive for both the individuals and taxpayers with respect to healthcare costs. Therefore, by screening embryos, we can save the government money.
To conclude, the screening of embryos is a very controversial topic with many valid points for and against.
We can screen embryos to detect whether the embryos have any genetic disorders such as cystic fibrosis. The screening of embryos involves taking a few cells from the embryo and analysing the genetic information to see if there are any genes for genetic disorders present. We can screen embryos from IVF (fertilisation in a lab) and from embryos in a womb.
If the embryos do have any genetic disorders, the embryos from IVF will probably be destroyed and the embryos inside a womb may be terminated (the pregnancy will end and a child won’t be born). It is because of these reasons that the screening of embryos is extremely controversial, especially amongst religious individuals who believe that life starts when a sperm and an egg fuse together to form an embryo; these individuals probably class the implications of embryo screening (destroying the embryo during IVF and terminating a pregnancy) as murder. Also, the screening of embryos implies that some genetic disorders are undesirable, which creates conflict and prejudice. Furthermore, individuals may want to screen the embryos for more than just genetic disorders; for example, screening the embryos for hair colour, eye colour etc… However, at the moment there are laws that prevent this from happening; currently, parents cannot even know the sex of the offspring (unless the sex influences the health of the offspring). A final negative is that screening embryos is quite an expensive process.
The positives of embryo screening are that genetic disorders reduce the quality of life for many individuals. Therefore, embryo screening can prevent babies being born with genetic disorders, which can reduce suffering. Furthermore, the treating of these genetic disorders is very expensive for both the individuals and taxpayers with respect to healthcare costs. Therefore, by screening embryos, we can save the government money.
To conclude, the screening of embryos is a very controversial topic with many valid points for and against.